Platform thesis
Behavior change is not a campaign.It is a daily substrate.
Most adherence products optimize the wrong variable. We treat behavior the way Stanford's B. J. Fogg taught us: as a function of motivation, ability, and prompt, designed across all three, every day.
Below is what that looks like in practice. Five levers, the research behind each, and a short note on what we deliberately don't promise.
The framework
Behavior = Motivation × Ability × Prompt
B. J. Fogg's Behavior Model (Fogg, 2009) says a behavior happens only when three forces converge in the same moment: a person is motivated enough, the action is easy enough, and a prompt arrives at the right time. Take any one away, even briefly, and the behavior doesn't happen.
Most wellness apps load up on motivation (cheerful copy, badges, push notifications). They under-invest in ability (make the action smaller) and prompt timing (when, not just whether). That's why their Day-7 retention crashes through the floor by week three.
Invyta is built across all three. Below: how each lever maps onto the model, and why we add a fifth force, social support, that the research treats as a multiplier on all three.
Behavior =
Motivation × Ability × Prompt
Motivation
cash · coaching · social ties
Ability
gamification · structure
Prompt
nudges · messages · alerts
“Tiny behaviors prevail when designers don't rely on motivation as the primary driver.”
01 · The prompt
Right cue, right time, no nag
A nudge, Richard Thaler and Cass Sunstein's term, popularized in their 2008 book (2008, Yale University Press), is any small intervention that shapes behavior without restricting choice. Default options. Reminders. Friction that's lower for the right action and higher for the wrong one.
Nudges are the most evidence-rich lever in digital health. Pop-Eleches and colleagues (2011) showed in a randomized trial that weekly SMS reminders increased antiretroviral adherence measurably in rural Kenya. It wasn't that patients didn't want to take their medication, but a prompt was missing at the moment of needed action.
Invyta's nudges are timed against the user's actual rhythm, not blasted on the hour. Reminders arrive when a behavior is plausible. Coaching notes appear when an advocate engaged, not as filler. The product treats attention like a finite resource.
02 · Motivation, kept warm
Coaching that adapts, not a chatbot pretending to be a clinician
Health coaching has a real evidence base. Meta-analyses across smoking cessation, diabetes self-management, and weight loss show coaching adds measurable improvement on top of standard care when it's structured around motivational interviewing (Miller & Rollnick, 2008) and brief, well-timed contact rather than dumping content.
Two patterns are well-supported in the literature:
- Implementation intentions: Peter Gollwitzer's (1999) research shows that prompting users to state when and where they will do a behavior (“I will take my morning dose at 7 a.m. at the kitchen counter”) roughly doubles follow-through versus general intent.
- Self-monitoring. Across diabetes and weight-loss trials, the act of tracking a behavior is itself an intervention. The data isn't only for the clinician: the act of recording reshapes the next decision.
Invyta's coaching is light and adaptive. It surfaces a relevant prompt when context warrants one. It doesn't impersonate a clinician.
“The strongest predictor of behavior change is not how much information someone receives. It's whether the right cue arrives in a moment they can act on.”
03 · Ability, made attractive
Streaks, calendars, and visible progress without leaderboards
Gamification has earned a deserved reputation for being applied poorly (slot-machine schedules, leaderboards, dark patterns. Done well, it's the lever that converts a hard behavior into a tractable one. Mihaly Csíkszentmihályi's flow research (1990, Harper & Rowe) and B. F. Skinner's operant conditioning work (1963) both inform what makes a behavior feel attainable: short feedback loops, clear progress, achievable next steps.
A heavily cited recent example in digital health gamification is Patel et al. (2019, JAMA Internal Medicine): a randomized trial in which families using a gamified step-tracking program hit physical activity goals at significantly higher rates than the control. The mechanism wasn't competition. It was shared accountability with predictable structure.
Invyta uses streaks (consistency), calendars (visible progress), and advocate visibility (chosen accountability). It does not use leaderboards. Public ranking systems crowd out intrinsic motivation, a finding from Self-Determination Theory (Ryan & Deci, 2000) that has held up across forty years of replication.
Clinically meaningful
In their randomized trial, Patel et al. found family-based gamification raised step counts versus control. We verify exact effect sizes for diligence materials.
04 · Motivation, with teeth
Cash works when points fail. The research is unusually clear
Why cash, specifically
Behavioral economics has spent forty years documenting two stable findings: people heavily discount future health gains (present bias, Loewenstein & O'Donoghue (1999), O'Donoghue & Rabin (1999), and others), and losses hurt roughly twice as much as equivalent gains feel good (loss aversion, Kahneman and Tversky's (1979) prospect theory).
Both findings have direct product implications. A small, near-term cash payment competes with the present bias against future health benefit. Framed as something the user can lose by missing a day, that same payment recruits loss aversion and outperforms gain-framed equivalents.
The headline studies
The cleanest demonstrations come from Kevin Volpp and colleagues at Penn's Center for Health Incentives and Behavioral Economics:
- Volpp, Troxel, Pauly, et al., 2009, NEJM: A randomized trial of financial incentives for smoking cessation found participants offered structured payments quit at substantially higher rates than the information-only control. The effect held at 12-month follow-up.
- Patel, Asch, Rosen, et al., 2016, JAMA Internal Medicine: A randomized trial of physical activity incentives found the loss-framed condition (money you can lose by not hitting your goal) outperformed the gain-framed condition (money you earn by hitting it), even though the two groups received the same total dollars in expectation.
- Volpp, Loewenstein, Troxel, et al., 2008, BMC Health Services Research: Lottery-structured incentives outperformed deterministic payments during multiple warfarin-adherence trials because human probability weighting overweights small chances of large rewards (also a prospect-theory prediction).
How Invyta uses it
Invyta delivers real cash, not points and not deferred rewards. Sponsors set the budget. Participants see a transparent ledger with every action they completed, every dollar earned, every dollar paid out. Incentive frames are configurable per program: gain, loss, lottery, or hybrid, depending on what the cohort and the sponsor's CFO will support.
When sponsors ask whether the incentive will recoup itself, the modeling is straightforward. Research from Penn's Center for Health Incentives and Behavioral Economics, plus internal program data, gives us a defensible band of expected adherence lift to plug into ROI conversations. We share the assumptions in writing.
Sustainably higher
Quit rates in the incentivized arm versus control in Volpp, Troxel, Pauly, et al., 2009, NEJM, measured at program end. The effect attenuated but persisted at 12-month follow-up. We cite exact published figures under diligence, not placeholder ratios.
“A dollar today is more behaviorally compelling than ten dollars in a year, and a dollar you might lose is more compelling than a dollar you might earn. Health-incentive design that ignores either is leaving outcomes on the table.”
05 · The multiplier
Health behaviors travel through social ties
Christakis and Fowler's 2007 NEJM paper, The Spread of Obesity in a Large Social Network Over 32 Years, sent shockwaves through population health when it documented that health behaviors propagate measurably through social networks. Subsequent work has shown the same for smoking cessation, exercise, and even subjective well-being.
The implication for product design: who supports a behavior matters as much as how the behavior is structured. Invyta's advocates feature lets a participant invite people they already trust (a parent, a partner, a friend) to see their progress. Advocates see what the participant chose to share. They do not see clinical data.
The research literature is firm on one point that's easy to get wrong: chosen social support helps. Assigned social pressure does not. A buddy you picked is a multiplier. A care manager you didn't pick is, at best, neutral.
“Social network effects on health are not metaphorical: they are statistically robust and bidirectional. Networks transmit risk and resilience alike.”
From thesis to product
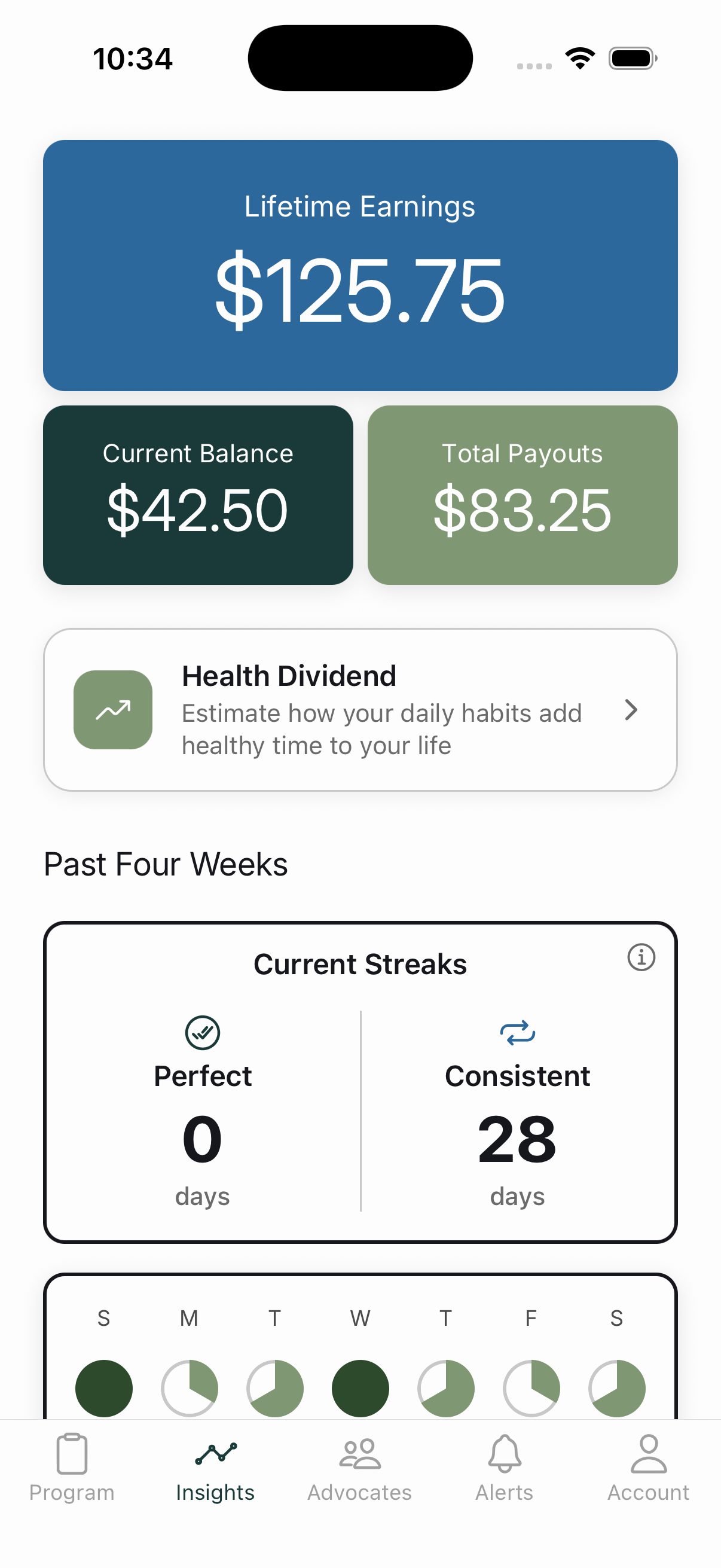
All five levers, on one screen
Insights is the screen where the levers stop being abstract. Lifetime earnings (the cash incentive made tangible). A 28-day calendar (visible progress, the gamification mechanic). Streaks (consistency feedback). Per-behavior breakdown (self-monitoring). It's the receipt for the work, and the place where participants realize the product is keeping its promises.
The moment
GLP-1s, payer reevaluation, and participant privacy expectations all changed in the last 24 months
GLP-1 therapies reshaped who needs persistence support: large populations now interact with chronic-care medications they didn't take three years ago. At the same time, employers and health plans are reevaluating digital point solutions and consolidating around platforms that can show daily, not monthly, engagement. And participants increasingly bring bank-grade UX and privacy expectations to any app that touches health.
Where we're headed includes deeper support for specialty cohorts, condition-specific program templates, and tighter integrations with payer and pharmacy data. Always with the same bar: daily use participants can sustain and sponsors can defend in committee. We will not promise dates on a static marketing page.
What we don't promise
Behavior change is probabilistic. Anyone selling certainty is selling a deck, not a product
Three things we say plainly, because they distinguish careful operators from marketing-driven ones:
- Engagement is not universal. Across every behavior-change literature we draw from, a real fraction of any cohort will not engage durably. Our reporting reflects that reality. Attrition is published, not buried.
- Effects attenuate over time. Volpp's smoking-cessation effect, Patel's gamification effect, and Pop-Eleches' SMS effect all weaken after the active intervention ends. We design program durations, taper schedules, and follow-up incentives with that in mind.
- Causality is hard. Observational adherence data tells us less than randomized data. When sponsors model ROI with us, we flag which numbers are causal estimates and which are correlational.
The honest version of “behavior change works” is that it works probabilistically, with measurable but bounded effects, and the product around it has to keep earning the user's attention. Anyone selling a deck without those three caveats is selling certainty that doesn't exist.
References
Full reference list
The citations above map to primary sources and standard texts in behavioral science and health economics. For the complete, ordered bibliography, see the full list of references in the Invyta white paper (PDF).
Model the ROI
Stress-test incentives with your CFO
Our calculator exports the vocabulary finance and clinical teams share before legal spends weeks on paper.
Open Savings Calculator